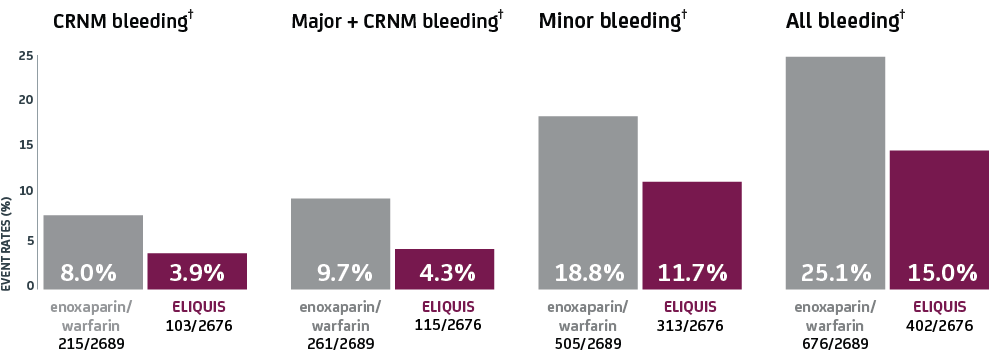
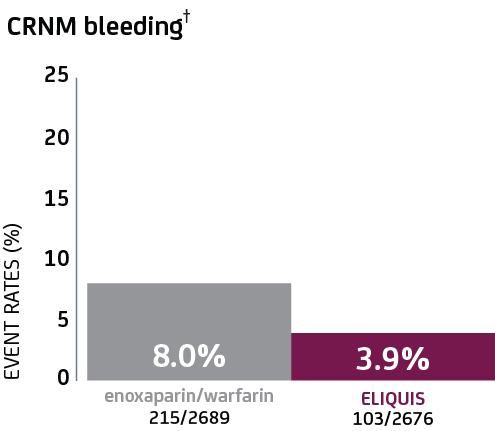
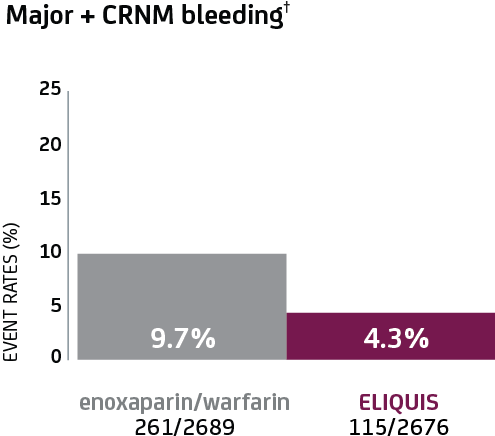
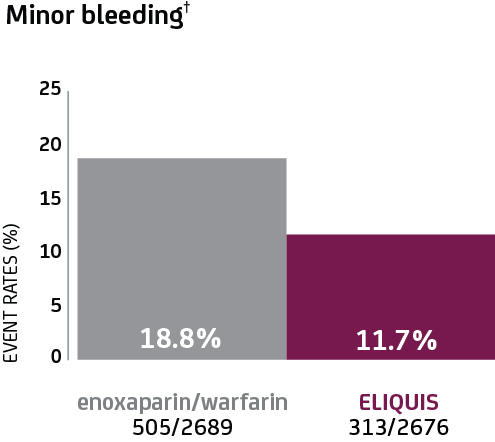
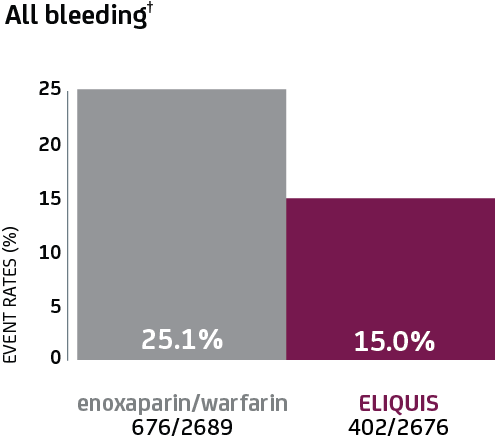
ELIQUIS demonstrated fewer bleeding events across key
secondary endpoints, including clinically relevant
nonmajor (CRNM) bleeding1†
ELIQUIS increases the risk of bleeding and can cause serious,
potentially fatal, bleeding.1
-
In AMPLIFY, the discontinuation rate due to bleeding
events was 0.7% in the ELIQUIS-treated patients compared
to 1.7% in the
enoxaparin/warfarin-treated patients1
CRNM bleeding was defined as overt bleeding not meeting the
criteria for major bleeding but associated with at least 1 of
the following: medical intervention, contact with a physician,
interruption of the study drug, or discomfort or impairment in
carrying out activities of daily life.2
Select examples of CRNM bleeding2
-
 Any bleeding leading to hospitalization
Any bleeding leading to hospitalization
-
 Macroscopic gastrointestinal hemorrhage, including at
least one episode of melena or hematemesis, if clinically
apparent with positive results on a fecal occult-blood
test
Macroscopic gastrointestinal hemorrhage, including at
least one episode of melena or hematemesis, if clinically
apparent with positive results on a fecal occult-blood
test
-
 Epistaxis lasting >5 minutes, that was repetitive, or
that led to an intervention
Epistaxis lasting >5 minutes, that was repetitive, or
that led to an intervention
-
 Macroscopic, spontaneous hematuria or hematuria lasting
>24 hours after instrumentation of the urogenital
tract
Macroscopic, spontaneous hematuria or hematuria lasting
>24 hours after instrumentation of the urogenital
tract
-
 Hemoptysis (if more than a few speckles in the sputum and
not occurring within the context of PE)
Hemoptysis (if more than a few speckles in the sputum and
not occurring within the context of PE)
-

-
Any bleeding compromising hemodynamics
-
Any other bleeding type considered to have clinical
consequences to a patient
















